Earlier I argued that trans* is not a disorder and that the problem is more likely with transphobia than with gender variation. I showed how much we are stuck in binary thinking that needs to get rid of its expectations of universality. A way out may lie in the concept of “fuzzy sets”. In the future, trans is in the head.
Who enters into combat against the idea that trans people would have a mental disorder, would best give perspectives for another way/outcome/solution. That is why we look amongst others to Ecuador.
In the end the battle for trans rights is not about identities, One should be able to freely live the gender identity one feels comfortable with. Since we have a basic right to identity, this should not lead to so many issues, we should be able to continue building a lovely en just world. Alas the struggle for identity (instead living and celebrating identity) is being used in a power struggle to privilege a particular conservative morality. The fight for identity is only a small and bloated (inflated) part of a broader struggle for justice. Though not everyone makes that step from acknowledgment to further action.
Only a small group of the trans* population enters (medical) transition. Some 12,5% in the Netherlands. Many do not because they do not want to, do not dare or just cannot. Some love comfortably in two genders or fluctuate between two genders, others again just don’t take gender as a reference point anyway. Gender queers who throw the system over board in that sense don’t have much with identity struggle either. Except that you must be able to be or to become whoever you feel to be. Afterwards: shall we now continue to change/improve the world?
Some good developments in the direction of autonomy and respect come from the Spanish speaking world. More and more you encounter the term “trans en la cabeza” there, “trans in the head”. That idea leads to a totally different, not by default male or female, gender expression. oftentimes no medical intervention either which in turn has to do with archaic and arrogant treatment y psychiatrists, that mostly check if you are “trans enough”. Partially this (trans in the head) is rather sub-cultural, partially it is mainstream.
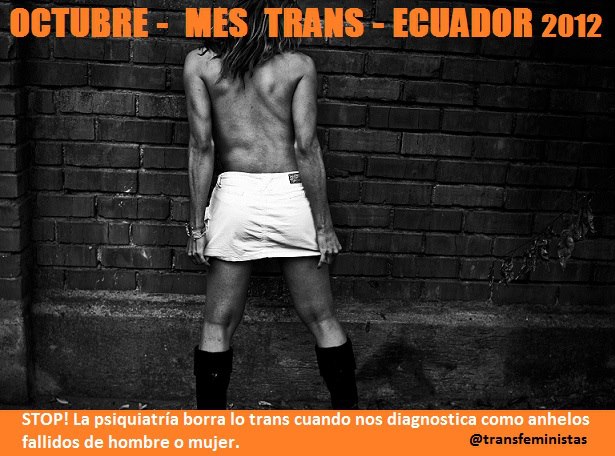
In Ecuador mostly trans people so seek medical assistance, be it official or not. Apart from the ID card that needs to be adapted to the gender one lives in. For that a campaign is waged these days, titled “Si es mi cédulo, tien que ser mi género”, “My ID must read my gender”by the organization “Cuerpos distintos, derechos iguales” (Different bodies, same rights). They warn for colonial concepts when the psychiatrist presses forward western ideas of how masculinity and femininity. In this sense the struggle for trans rights fits well in current anti colonial struggle.
This leads to a multitude of bodies and identities and thus to an explosion of what we understand by “men” and “women”. A revolutionary development: less than ever identity will relate to being born in a certain body and more to a certain conviction. Also it is a revolutionary appeal to the human right of autonomy of the body. So revolutionary alas that frequent and fierce resistance of the gender powers that be is to be expected. Nevertheless this is the way forward and we are on our way.
The current health care model for trans * people many times is defended as protecting the patient. Protecting them against regrets. A physician wants to be sure the patient they see, is serious, is not acting on impulse. This worry we can understand, the solution however is wrong.
A large part of the worries that physicians have regarding autonomous trans people comes from fear and ignorance. Fear of loss of work and also loss of authority.
Fear of people taking decisions they will later regret and will hold the doctor responsible for. Only to bring them before the disciplinary board. That is traumatic for the physician, when they have done their best to deliver a good job on explicit request. Incomprehension because they do not understand trans* people. They haven’t learnt a thing about them during their studies of psychology, psychiatry or medicine. And if something is taught, that is mostly rather out of date. Only this year thinking progressed slightly with the introduction of the new DSM and a new nomenclature for trans* issues.
A trans* patient does not need more or different protection than a non-trans* patient. Just as a Swedish patient needs no more or better protection than a French one. Where a doctor cares for the mental health of a patient because they do not appear to be stable, this mental stability is the problem. Not the being trans* of the person. The question should be: If I would have a patient with an appendicitis, or for cancer surgery, would I also require a psychologist’s certificate about their well-being? The fact that something is culturally loaded, is not enough reason to as for extra intervention/extra control.
Also everyone has a right to regret. However cynical that may sound. It is very well possible a trans* person who comes out is not sure of themselves. Identity develops. The same with gay and lesbian and bisexual people. Many times they are not coming out because they feel so great with the idea. Often they only do so when a lover is in sight, although they feel their being different for a much longer time already. They don’t need to see a psychologist, they have no longer a disorder (since 1991). Not coming out, living a non-authentic life, is something you can regret also. Like you can regret marrying, or not marrying. Or having children, or deciding not to have them. No one can tell if things will work out the way it was intended. So I would almost state: also trans people have the right not to be happy with their life and their choices. It is anyway not up to the state or the medical profession to always try to prevent us from failing, from regretting. Or should we also send prospective parents first to a psychologist or sexologist? Prospective spouses to a marriage counselor to have their love tested on stability, on longevity?
That fear we would decide for ourselves, for prosecution because they helped the ‘wrong’ trans person also stems from fear and ignorance. First of all, informed consent should be a requirement. With or without a psychologist, if the patient doesn’t understand what is involved, at is where it ends. Secondly, it won’t be the first time a medical psychologist would be involved when a patient has to undergo invasive treatment. But not all patients that undergo say oncological treatment will have to see a psychologist.
When society stops freaking out about trans* people, the suffering will decline enormously. After all, it is the outside world that gives us a lot of our trouble. And we as a part of that world got the message that it is not good to behave as we do, to feel like we do. So, stop freaking out and join the revolution. We are nothing more than a threat to your mental status quo. So what.
(Translation of “allemaal angst”, that appeared here on 21-12-2013)
Ik hoor het huidige zorgmodel voor transmensen nogal eens verdedigd worden met het argument dat men de patiënt wil beschermen. Behoeden voor fouten. En ook dat een arts zeker wil kunnen zijn dat de persoon in kwestie het meent en niet in een opwelling besluit. Nou is die angst begrijpelijk, maar de oplossing is dat niet.
Eigenlijk komt een groot deel van de zorgen van de medici voor autonome transen voort uit angst en onbegrip. Angst voor verlies aan werk en autoriteit ook. En zeker ook angst voor mensen die besluiten nemen waar ze later op terug komen en waarvoor ze dan vervolgens de arts voor de tuchtraad slepen. Dat is traumatisch voor de arts, wanneer deze zhaar best heeft gedaan goed werk te leveren op expliciet verzoek.
En onbegrip omdat men transmensen niet begrijpt. Men heeft er niets over geleerd tijdens de studie pyschologie/psychiatrie/geneeskunde. En meestal is dat wat men eventueel leert erg achterhaald: pas dit jaar is het denken officieel wat opgeschoven met de nieuwe DSM.
Een trans* patiënt hoeft niet beter beschermd te worden dan een niet-trans* patiënt. Zoals een Franse patiënt niet beter beschermd hoeft te worden dan een Nederlandse. Wanneer een arts zorgen heeft omtrent de geestelijke gezondheid van de patiënt omdat deze niet stabiel overkomt, is die geestelijke stabiliteit het probleem. NIet dat die persoon trans* is. En dan dient men zich af te vragen: als ik een zwaar bezorgde patiënt voor een blindedarm ingreep, of een kankeroperatie binnenkrijg, zou ik daarbij ook eerst van een psycholoog een verklaring omtrent zhaar welzijn willen? Dat iets cultureel beladen is, is nog geen reden om extra controle te vragen.
Verder heeft iedereen het recht op fouten. Hoe cynisch dat ook moge klinken. Maar het is goed mogelijk dat de trans* persoon die uit de kast komt niet zeker is. Identiteit ontwikkelt zich ook. Holebi’s zijn ook vaak helemaal niet zeker als ze uit de kast komen, en doen dat vaak pas als ze een vriend/in/g krijgen, terwijl ze hun anders-zijn al veel langer voelen. ZIj hoeven niet langs de psycholoog, zijn niet meer ‘ziek’. En van niet uit de kast komen, niet waarachtig leven, kun je ook spijt krijgen. Zoals van trouwen, of juist niet trouwen. Van kinderen krijgen, of juist niet aan kinderen beginnen. Wie zal zeggen dat het altijd goed gaat? Ik zou bijna zeggen: ook transen hebben recht op ongelukkig zijn, op fouten maken. En het is zeker niet aan de staat of de medische wereld ons daar per definitie voor te proberen te behoeden. Of moeten mensen die kinderen willen ook eerst langs de psycholoog of de seksuoloog? Wie gaat trouwen langs iemand die hun liefde test?
Wat betreft die angst voor zelf besluiten, voor vervolging omdat men ‘de verkeerde’ heeft geholpen: daar zitten een paar rare dingen aan. Ten eerste, is informed consent dringend gewenst, een voorwaarde zelfs. met of zonder psycholoog, als degene om wie het gaat niet snapt waar zhe mee bezig is, houdt het verhaal überhaupt op. En ten tweede, voor ingrijpende medische behandelingen wordt een patiënt wel vaker langs een medisch psycholoog gestuurd.
Wanneer de samenleving ophoudt spastisch te doen over trans*mensen zal het lijden ook sterk afnemen. Tenslotte wordt het lijden voor een groot deel veroorzaakt door hoe de wereld tegen ons aankijkt. En wij als deel van die wereld hebben opgepikt dat het niet goed is om zo te zijn. Stopt met spastisch doen en join the revolution. Wij zijn hooguit een bedreiging voor je mentale status quo. Zut alors.
The press release of the Amsterdam gender team they sent out on Wednesday December 18, stating they cannot treat all the people who applied in recent times constitutes a brilliant opportunity to stop diagnosing trans people with gender dysphoria and start an informed consent based treatment process.
The day after the glorious victory of the passing of a strongly improved gender recognition law in the Netherlands, the Amsterdam Gender team that treats 85% of Dutch trans people who need a bodily and/or legal gender change, published a press realease saying they may stop accepting new patients within half a year. Where there is an increase of 500% of applications in recent times, they do not get enough extra money to help them.
Of course this a bad development. When health care cannot be delivered people lose their right to health on certain points. On the other hand, with the attention because of the adoption of the new law, this is a form of blackmail. A way to hopefully get government and insurance companies around the table. Completely legitimate.
But as usual there is a back story to this. Dutch government designated the VUmc team as the Expert Centre on transgender Health in the Netherlands. And persistent rumours have it they use this position to create an oligopoly, having only the UMCG in Groningen that caters for the northern provinces, as their collegial competition. A small department at LUMC in Leyden treats trans* children.VUmc actively discourages surgeons or endocrinologists working elsewhere to treat trans* people. When psychologists elsewhere want to diagnose trans* people so they can have their bodily and legal changes, these are also discouraged.
I do no tell this to badmouth the work they do. This means to explain part of the origin of the problem. And probably from their point of view it is completely legitimate. So they need a good solution. Well, that is easy. Tell the psychologists to stop diagnosing their “patients”. That will save millions of euros.
Alternatively a better way of spending the money they got and the money they still need, lies in helping trans* people cope with the transphobia they experience. And with their internalised transphobia they develop from all the bad reactions. Psychologists are good at helping people get rid of many complaints and otherwise learn them cope with other issues. Transphobia (society’s reaction to people who do not fall within the accepted limits of male/female) causes depression and anxiety and more. Suicidal tendencies. That needs to be helped. But diagnosing trans people with gender dysphoria (DSM-5) or gender identity disorder (ICD-10) or gender incongruence (ICD-11, proposal) does not work. I imagine these psychologists would be far more proud of their work also, would feel more qualified ease these complaints than diagnose people with a non existing disorder. Additionally it will still be cheaper since not everybody needs this help.
In the early morning of the 18th of December 2013 the Dutch Senate passed the proposal for updating the existing legislation of now 18 years old. It has been a long and bitter fight, in which some core demands have been realised, but it is not over yet. Continue reading “Trans law in the Netherlands passed. Now what?”
For some time now the German decision to require parents of a child with ambiguous genitals to register their child without a sex marker and without protection or time limit, is making the news. To the growing displeasure of intersex activists.
Displeasure because intersex activists have not been consulted and if consulted would have advised against this law. Because of the utter confusion about a “third gender” or “third sex”. Because the way it works, parents and doctors will be inclined more to cut up the childs genitals instead of less. Without education or protection: who wants a sex ambiguous child?
To first tend to the misunderstanding about Germany that the press still furthers. Germany does not have third gender option. Not even or intersex infants. If a child is born in a German hospital (or at home) and on grounds of the genitals its se cannot be defined without a doubt, the requirement is to leave the sex marker (gender marker) open in the birth certificate. There is no time limit to it.
Where the power to decide on the childs sex lies in medical hands the tendency will be to try to prevent any ambiguity, out of professional pride (“Look! We can fix this!”). Be it through prenatal hormone therapy (with certain intersex conditions the mother gets off-label prescription of dexamethasone), surgical or postnatal hormone treatment prescription Or even abortion. Preimplantation Diagnostics and other screenings are unwelcome interventions where it concerns intersex “discovery”.
This will not help prospecting parents in handling the body diversity of their child. The most friendly it will be frowned upon and run into problems when for example registering it for Kindergarten. Given the ttal lack of support in society, the enforcing of a sex and gender binary everywhere in life, already the child’s start will be complicated. How will it be treated by family (“we don’t now what it is”), in Kindergarten where everything is pink and blue ..
The way it works, intersexed children (they fit within a diversity of bodies, but through medical scrutiny they intersexed, made intersex or having a “Disorder of Sex Development” to make it worse) only get the worst of possibilities, not the best.
Would anti-discrimination legislation help then: Well, yes. Though there is a risk of making thngs more complicated to keep the system. Instead of creating a limited extra category, German government could have had the courage to open it up for everyone to have no sex/gender marker in the birth certificate and other documents. At least let it die out. So that from end 2013 all children would be free of a sex/gender marker, and after some years that population will have grown and gender registration starts dying out with the deceased.
A word about terminology here: usually we speak of gender marker, but it happens at birth on the view of the genitals of a baby. The “no sex marker” solution the german chose and others are eyeing, shows that sex and gender are constantly conflated. Because of specific genitals, a specific gender identity and gender role is attributed too the child. naturalistic thinking with biologistic arguments then takes care of the rest: your gender is supposed to stay the same through life, apart from errors. in classic legislation the legal problem trans people present is solutioned along these “error” lines. Apparently the person develops differently than we expected, so we grant the right the correct this error. Another reason the Argentinean solution for gender recognition is so revolutionary.
The solution to havng a two option system and people that do not fit in can theoretically be solutioned by introducing a new category, or leave the field open. But that leaves two important questions: is it the best solution, and waht do the people involved say of it? There is a saying “Nihil nobis sin nobis”, nothing about us without us. Decent politics involves the group that has to benefit or suffers from a certain solution. This has not happened here. Elsewhere, in the Australasian region third gender solutions have been introduced through the explcit wish of part of the population. Not in Germany however.
What would be the best solution to the problem of having non fitting categories? One could opt for opening up a real third sex/gender category, indicated with an X on all official documentation (this is the internationally recognized solution from the ICAO). But for legsilation there must be a need and it must be proportionate in its effect. In Europe (Council and Union) there also is the equality principle. New categories , new distinctions may only be introduced in legislations where equalilty is protected. In Germany this is definitely not the case, neither in Australia where inter* people cannot marry a man or a woman since they are not one. The very least to do is introduce protection against discrimination. If not it is a solution on unequal footing and against the equality principle.
Next there is the risk of wanting to create even more categories. Why not one or inter* and one or trans*? Sensile lawyers will rejext this idea since it makes no sense to discriminate between so many not really essential traits. Which in turn brings us to the question: if continuing to create categories is senseless, do the existing categories make sense? Does sex registration in the civil registry make sense? Medically speaking, sex registration might make sense. But the civil registry is not for medical information. With equality legislation covering more and more terrain, inequality between men and women seen as a somewhat retarded way of thinking (although still very much alive), what is the use of registering? Just because bodies are different and they have different roles? That is hardly a good argument.
The best way then is to simply abolish sex/gender registration at the civil registry. Make those categories moot, uninteresting, without importance. It is not about abolishing men and women ro male and female identities, it is just about quitting to enforce them. Most reasons to keep the status quo come from the same realm as objections against marriage equality between genders or the possiblity to change genders, sc. moral conservatism.
Of course between act and dream stand laws and moral objections – to quote the Dutch poet Willem Elsschot – but that should not be insurmountable.
From midnight tonight six trans* activists In Andalusia, Spain will start a permanent hunger strike until either the bill for better trans legislation that is stuck, will be really introduced in Parliament or until they die. Continue reading “Spanish trans activists start hunger strike”
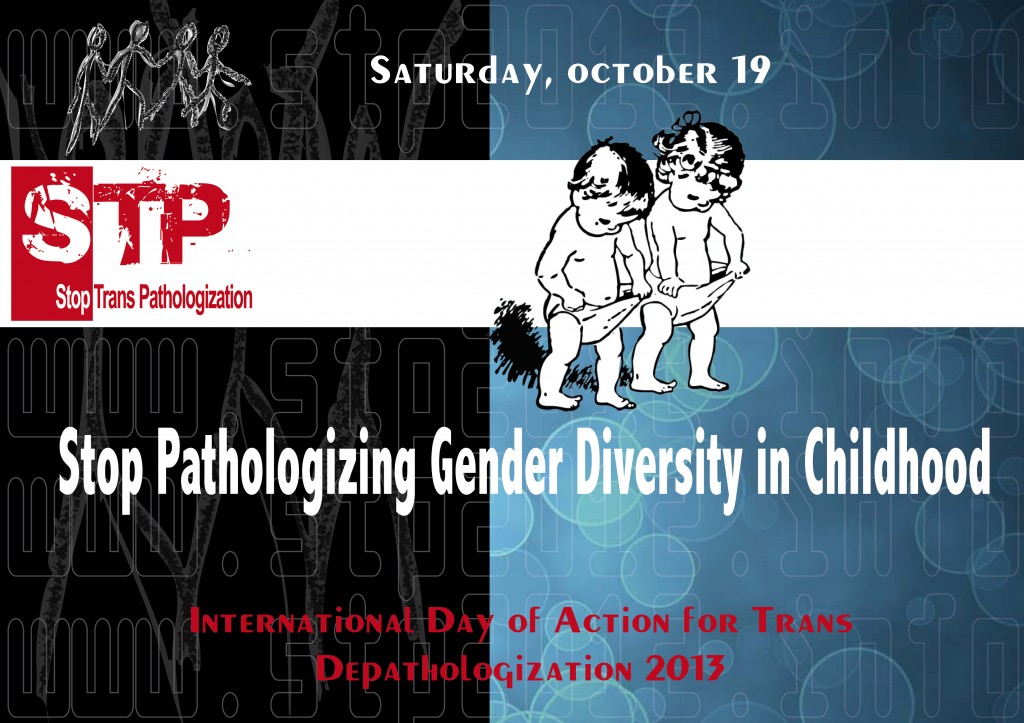
October 19, 2013 is the international day on the depathologisation, declaring not a disorder but a positive diversity, of trans people. And because of high level developments in the World Health Organisation, that is responsible for revising the International Classification of Diseases, that is used for understanding what is a sickness, a disease, a disorder – be somatic or psychological. This is a global Classification – unlike the DSM that is still mostly US based but having a wider use. Here in NL psychologists use it, health insurers use it. For adolescents and adults there is a positive change going on, although the battle is not yet won. Because of this last issue, introducing a diagnosis for children, and 2014 being a decisive year for the new ICD, the pathologisation of trans children has been chosen as the theme for this year.
The suggestion for a theme usually comes from Spain where the campaign started in 2009. It was the time that the process to change the DSM started and they started to create global awareness for the changes. After all: the DSM still declares trans* people having a mental health problem. And when the process to change the ICD got under way, this had been taken into the campaign. Nowadays a strong focus of advocacy for trans health lies in getting a good description in the ICD-11. Since that will be decisive for how many people in the medical and political world will see us. If trans people are not (mentally) ill, but instead suffer from society, we will be taken more seriously. So that is why today and why the theme.
What is today about?
I will first define the situation: gender kids are not welcome as who they are, most learn to hide very early in life. I have recent data from the UK on that. Next I will give an overview of several developments in the social and the medical world. I will focus on how the big international classifications that are in use. By that I mean the infamous Diagnostic Statistical Manual of menatl disorders (DSM, version 5) of the American Psychiatric Association (APA) and the global, more responsible International Classiication of Diseases (ICD, version 10) of the World Health Organisation (WHO). Developments there are going in the wrong direction. And that has pretty much to do with it being children and with queerphobia.
Also I will give an update on developments in the Netherlands; what support is there, how are parents reacting? What does the clinic do? What would be good ways to advance our case for gender freedom?
Trans*
To start with trans*: this is not just transgender in the transitioning variant. It can surely mean transgressing gender norms, being and behaving gender non conforming. Because trans* is who trans* does. In a way many of you are also trans*: you do trans*, you transgress gender norms. Don’t come to me “Hey, but I’m fine with my body”. That is just one version of gender diversity, of trans*. Being trans* does not require gender dysphoria or gender incongruence or however you call it. And trans* is not just identity, it is also expression. Since so much what we all gay or lesbian or bi, is more gender expression than sexual orientation or gender identity.
So trans* can be anything non gender conforming. And acceptance for that already is quite low for kids. While the Netherlands may be relatively tolerant of it, and many young parents seem to be, recent UK data show that also the seemingly more accepted tomboy behaviour of girls and non apparent trans boys is not really accepted. Non-apparent then stands for people who later in life tell to be trans already from early on but didn’t tell anybody back then.
Kids
And by kids I mean children before puberty hits them, which roughly mean between 10 and 12 years old. Usually one says: puberty starts with Tanner stage 2. Then physical changes start appearing. In the Netherlands that gets ever earlier, and in several other countries also.
Although it is a generally accepted idea that children change, that change and development are the core phenomena of a child’s life, many implicit norms govern this period. A good example is that there is an Amsterdam kindergarten where children of many gay and lesbian parents spend their day. The personnel are very happy with the lesbian and even more with the gay parents. However all the kids are neatly divided in boys and girls and treated differently. I think this has much to do with idea that being gay and lesbian is seen as only a relationship thing, a sexuality thing, something private. Gays can be great parents also! But this goes completely beyond the point that so much is gendered behaviour, based on gender identity and/or expression.
Sterlisation is for cats, not for me
ICD
It is clear that the Committee that manages the chapters relevant to trans people is convinced gender identity issues must be relabeled en get a different position. The name is in the process of being changed from “Gender Identity Disorder” to “Gender Incongruence”. A mismatch between body and felt identity. That is better already, better also than Gender Dysphoria. But:
Why must there be such a diagnosis? The gender identity is not wrong, just different.
Being non trans*, the default situation of being cisgendered, still is the definition of Normal
A new diagnosis is being introduced that concerns trans* children. So a child living differently is still bad, wrong
It is the WHO that decides through scientific research what is to be considered a sickness, illness or disorder. Everything health related is in their remit. For the description of diseases etc. there is the International Classification of Diseases, ICD for its abbreviation. It is going to version 11 now, after the longest time between versions. ICD-10 is from 1990 and got in to function in 1994. Since 20 years is a long long time, the changes will be drastic, and many things will change: biomedical sciences have advanced enormously and everything may be streamlined more than before. So it will also be in things transgender related.
But the WHO is not only purely scientific and apolitically health care related. LGBTI issues face enormous contention from the usual suspects of human rights refusers for LGBTI people: the Vatican, the African group Russia and some consorts, several countries united in the Organisation for Islamic Cooperation. Recently there was to be a discussion about discussing LGBTI health issues and the issue got removed form the agenda thanks to pressure from these countries. For now the tendency within WHO is to declare it a technical issue and remove it from the agenda because of too fierce resistance.
Trans identity issues are now going from the horrible: Gender Identity Disorder” to most probably “Gender Incongruence”. The DSM 5, that American horrible psychiatric classification uses gender dysphoria. Incongruence is the least harmful term of the three, but still does not take its departure in gender diversity with all gender identities equally valid. So tis still not good. Gender dysphoria means one has lots of stress, anxiety, depression because of ones trans identity. Which is another case of wrong angle: it is not the identity in itself that causes so much trouble, it is how the world reacts and how one learns to look at it. And you know already quite young if it is OK to live like you feel. Which is why many trans people only come out later in life. Lucky the people who have enough to support to come out young. And can more or less freely develop their identities.
Gender Incongruence only means that your body and your identity do not match, are not congruent. But that still is not good enough of course. It is doable and better than dysphoria, but still.
The bad new thing for this Classification is that suddenly trans kids*, those who are not adolescents, the K-12 kids, need a separate, autonomous diagnosis of their Gender Incongruence. It will then be called, gender incongruence in children. But there are a couple of strange or incorrect things with this.
An important detail to add is that the proposal is to have the diagnosis onl apply to those children with severe complaints. Not every kid with a non traditional gender expression would fall under it. Only those whith “severe incongruence” as I imagine the wording might be. The fear for gendernon conforming behaviour seems to lessen in these circles. because they aslo say this with adults adn adolerscents, lready in the DSM-5.
First and foremost: they are sort of de-pyscho-pathologising adults. Because adults will be in a separate chapter for gender identity stuff, or in a chapter on sexual health. Not any more in the current chapter (F.64) of mental and behavioural disorders. But since children below puberty cannot get puberty blockers, there is nothing medical with them, so diagnosing them is diagnosing their – changing and developing – identity, means putting them with mental health issues.
When there is nothing medical, there is no need for diagnosing. So it is irrelevant. Surely since psychosocial support can be arranged through already existing constructions. This way a new class of experts and of treatment will be created. And once created, a specialism doesn’t want to close down.
Situation of trans kids according to research
Since this is all about trans* kids, it would be good to know a bit more about how they live, what their problems are. The problem is: there is only very little research in this. And most comes form the medical/psychiatric division of society. Not only that, it comes from researchers with a strong agenda for normalization. A name to remember in this is Kenneth Zucker from Toronto. In Berlin, Germany there is professor Klaus Beyer working with trans* kids who also has clearly non respecting ideas. Don’t get your kids to the Charité hospital in Berlin if they are queer.
The problem with Zucker and his pal Richard Green is their disrespect for the autonomy of trans people. Green is the author of “The sissy-boy syndrome”. He is Zucker’s predecessor and together they try to make a strong case for reparative therapy. This means: attempt to -de-transgender the kids, to un-gay them. Because gay and trans is Wrong. And trans is worse than gay (that is at lest within the gender binary). In the Netherlands people like these do not work at the gender clinics, but they might run loose as independent psychiatrists. Which might be even more dangerous: if the parents don’t know about the gender clinic’s youth program or better about Transvisie Zorg, the child might suffer much.
Natacha Kennedy
From recent UK research by Natacha Kennedy we know that of the respondents to an online survey most were ‘non apparent” trans kids. That is: they felt different already early in life but came out far later because they knew it was not considered a good thing to be trans. Already at age 8 the social radar of all children is god enough to realize this. There is no majority of one type of trans* in this research: the respondents have come out as cross dressers, transgender, genderqueer, mixed gender. The consequence of this feeling already quite young to be apart, different form the others leads to the feeling of not being able to live as one wants, to invest a lot in a gender identity that is not one’s own.
That does not have to contradict our cherished idea that gender is doing. It appears many people who live one thing, slurp, suck in what they are actually more interested in. To quote Butler in this: “Femininity is thus not the product of a choice, but the forcible citation of a norm, one whose complex historicity is indissociable from relations of discipline, regulation, punishment.” (Bodies that matter). Anyone wonder about the appearance of “gender dysphoria” then?
This nonrecognition of gender diversity is something seemingly universal. Surely here in the Netherlands the idea of gender expression is not very developed in general discourse.
Support
So what is there in support? As it is said the Netherlands is doing very well in medical support for adolescents, the question of course is: what is there for the young one? Well, there is support from Transvisie Zorg that have a social worker and a sexologist who see the parents, visit schools, talk to schools, see the kids if they want. Most of their work is with the adolescents, but a growing number of parents call for support. Their list of visited schools grows at 40 schools per annum!
The most common phenomenon roughly from 10 on, is bullying. More girlish boys than boyish girls get bullied. However every school got protocols against bullying. When talking with schools Transvisie points at bullying and the need prevent this, but it is mostly up to the kid and their parents to go to school and tell the staff they get bullied.
And then there is the gender clinic that gives “temporary” diagnoses. Precisely in the idea the ICD want s to have that diagnosis: to make it easier to enroll in the adolescent program. How good the support is, depends very much on the quality and opinions of the psychologist.
From July 31 to August 2 the World Outgames LGBT Human Rights Conference took place in Antwerp. The conference was titled: “From safe harbours to equality. A changing LGBT world: transitions and migrations.” For a LGBT human rights conference I am sad to say it was an absolute failure for being not inclusive and run mostly by Gay Inc. The only good thing being mainstream gay being called out on racism. Continue reading “A gay rights conference in Antwerp”

 Xavier Héraud")


